heart - heart disease heart attack heart health blood vessels artery clogged lower cholesterol Why Our Arteries Become Clogged As We Age
The aging process damages blood vessels, even when conventional risk factors
such as cholesterol and blood pressure are within normal ranges.
Despite aggressive intervention with diet, exercise, supplements, and drugs,
pathological changes still occur in the arterial wall that predispose aging
adults to vascular diseases. The encouraging news is that a non-prescription
method has been developed to address the underlying reason why arteries become
occluded as people reach the later stages of their lives.
For the past 35 years, the standard way to treat coronary atherosclerosis has
been to bypass the blocked arteries. Recuperation from coronary bypass surgery
can take months, and some patients are afflicted with lifetime impairments such
as memory loss, chronic inflamThe scientific literature reveals that atherosclerosis is associated with
high blood levels of homocysteine, C-reactive protein, insulin, iron,
low-density lipoprotein (LDL), and triglycerides, along with low levels of
high-density lipoprotein (HDL) and testosterone. Optimizing blood levels of
these substances can dramatically reduce heart attack and stroke risk.
Prescribing a "statin" drug is what today's doctors typically do to prevent
and treat coronary atherosclerosis. Cholesterol and LDL, however, are only
partial players in the atherosclerosis process.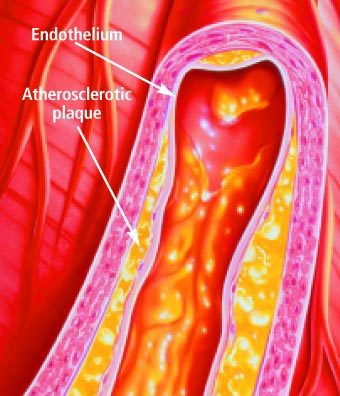
Anatomy of the Artery
Arteries are the blood vessels that bear the full force of each heartbeat.
Laypeople often think of arteries as flexible tubes whose only function is to
carry blood that flows continuously throughout the body. In reality, arteries
are dynamic, functioning muscular structures that in good health expand and
contract to facilitate circulation and maintain optimal blood pressure.
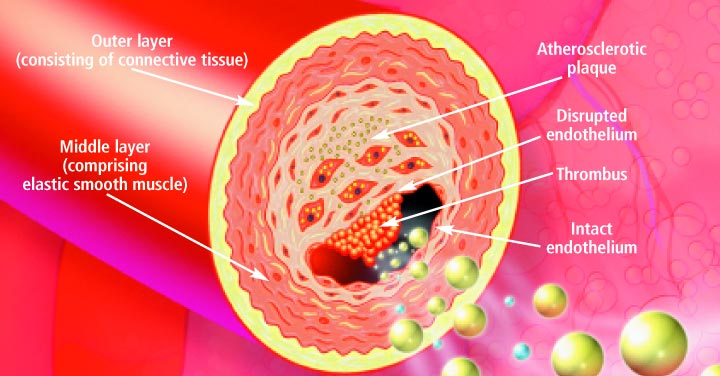
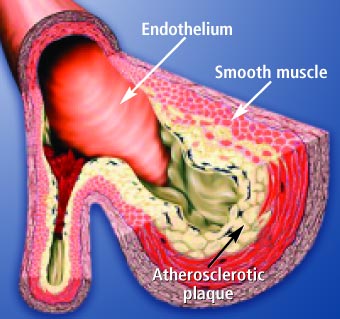
The artery's outer layer mostly consists of connective tissue and provides
structural containment for the two layers beneath. The middle arterial area
comprises elastic smooth muscle that provides the contractile strength to make
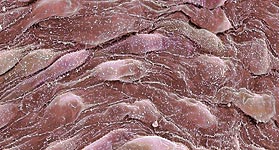
possible the artery's expansion and contraction with each heartbeat. The inner
layer -known as the endothelium- consists of a thin area of endothelial cells
whose integrity is crucial if atherosclerosis is to be prevented.
A vital function of the endothelium is to form a barrier to prevent toxic
substances in the blood from entering the elastic smooth muscle in the middle
vessel wall. Another specialized function of the endothelium is to react to
mechanical forces such as blood pressure and blood flow generated by the heart's
beating action. The endothelium releases substances into cells of the middle
layer smooth muscle that changes the tone or firmness of the artery.
When endothelial cells sense an injury, they produce signals that prompt
smooth muscle cells in the middle arterial wall to change. These changes result
in the smooth muscle cells moving toward the site of vascular injury, where they
reposition themselves just beneath the endothelial cell layer. In reaction to
injury, endothelial cells also produce substances that signal circulating blood
cells to stick to the endothelium (instead of effortlessly flowing through the
vessel). Atherosclerosis gradually forms in response to this initial injury to
the endothelium
Changes in the Aging Endothelium
As we grow older, some of the specialized functions of our endothelial cells
become blunted. The self-renewal process weakens. The endothelial barrier
becomes leaky. Signals to the middle wall smooth muscle cells that regulate
their function become altered.
Smooth muscle cells behave as if in reaction to endothelial injury, migrating
to the endothelium, where they multiply and produce matrix proteins that
gradually occlude the blood vessel. The addition of these smooth muscle cells
and matrix proteins within the sub-endothelial space results in thickening of
the artery's inner wall. In older arteries, the inner wall becomes a
battleground where multiple reactions occur that are similar to the process of
chronic injury. The inner wall dysfunction that occurs in the aging artery
provides fertile soil for the seeds of atherosclerosis. All of these processes
whereby normal endothelial function is compromised are collectively referred to
as endothelial dysfunction
How Atherosclerosis Develops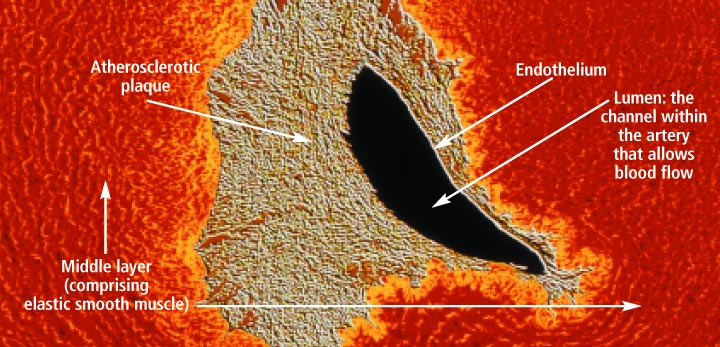
Atherosclerosis is so common in older adults that some experts used to think
it was part of normal aging. An alternative view is that atherosclerosis is a
disease process that takes advantage of changes that occur within the aging
artery.
The vascular aging process and atherosclerotic process influence each other
and become intertwined as we age. The more severe vascular aging is, the easier
it is for atherosclerosis to take hold. The more severe atherosclerosis is, the
greater its impact on diseases associated with vascular aging, such as stroke
and heart attack. Thus, it appears that with advancing age, atherosclerosis and
the aging process combine forces.
An often-used analogy for atherosclerosis is a "clogged pipe". This misguided
perception either leads to bypass surgery or a procedure in which the blocked
coronary artery is forced opened with a balloon catheter (angioplasty) and a
stent is implanted to keep the artery open. While these surgical procedures have
become necessary for many people, the "clogged pipe" analogy is an inaccurate
way to view the process of atherosclerosis.
 The
Arterial Wall Under Attack The
Arterial Wall Under Attack
High blood pressure, elevated LDL and triglycerides, low HDL, cigarette
smoking, diabetes, obesity, and lack of exercise contribute to endothelial
dysfunction and the subsequent development of atherosclerosis.
Additional endothelial-damaging factors include excess levels of glucose,
insulin, iron, homocysteine, fibrinogen, and C-reactive protein, as well as low
HDL and free testosterone (in men).
Homocysteine is particularly dangerous because it can induce the initial
injury to the endothelium. Homocysteine then facilitates oxidation of the fat/LDL
that accumulates beneath the damaged endothelium, and finally contributes to the
abnormal accumulation of blood components around the atherosclerotic lesion.
Fibrinogen is a clotting factor that accumulates at the site of the
endothelial lesion. Fibrinogen may contribute to plaque buildup or participate
in blood clot-induced blockage of an artery after an unstable atherosclerotic
plaque ruptures.
Glucose at even high-normal levels may accelerate the glycation process that
causes arterial stiffening, while high-normal fasting insulin inflicts direct
damage to the endothelium.
High levels of iron promote LDL oxidation in the damaged endothelium, while
low levels of testosterone appear to interfere with normal endothelial function.
Propionyl-L-Carnitine (PLC)
Research suggests that propionyl-L-carnitine (PLC) plays an important role in
protecting the function and health of endothelial cells. Studies also indicate
that PLC may act as a nutritional corrective agent, relieving clinical symptoms
of cardiovascular conditions such as peripheral arterial disease, angina,
coronary artery disease, cardiomyopathy, intermittent claudication, ischemic
heart disease, atherosclerosis, and congestive heart failure. PLC appears to be
more potent than L-carnitine in improving vascular function.
PLC passes across the mitochondrial membrane to supply L-carnitine directly
to the mitochondria, the energy-producing organelles of all cells. Carnitines
are essential for mitochondrial fatty acid transport and energy production. This
is important because heart muscle cells and endothelial cells burn fatty acids
rather than glucose for 70% of their energy. By contrast, most cells generate
70% of their energy from glucose and only 30% from fatty acids.
 Carnitine
deficiency has been associated with congestive heart failure. PLC
supplementation has been reported to increase exercise capacity, optimize energy
production, and reduce ventricular size in patients with congestive heart
failure. Carnitine
deficiency has been associated with congestive heart failure. PLC
supplementation has been reported to increase exercise capacity, optimize energy
production, and reduce ventricular size in patients with congestive heart
failure.
The myocardium, the muscular substance of the heart, comprises cells called
cardiomyocytes. A study of cardiomyocytes found that PLC helped to correct an
imbalance between the production and utilization of adenosine triphosphate
(ATP), the energy currency used throughout the body. This suggests that PLC may
improve cardiac performance by improving energy metabolism and optimizing ATP
levels.
The endothelium is the thin barrier that separates circulating blood from the
smooth muscle interior of the artery. Healthy endothelial cells help to maintain
a normal cardiovascular system. Aging, poor lifestyle habits and nutrition can
lead to endothelial problems.
Propionyl-L-Carnitine (PLC) plays an important role in protecting the
function and health of endothelial cells. PLC passes across the mitochondrial
membrane to supply carnitine directly to the energy-producing organelles of all
cells. Carnitine is essential for mitochondrial fatty acid transport and energy
production. This is important because endothelial cells burn fatty acids for 70
percent of their energy.
Adenosine triphosphate (ATP) is a critical component of the cellular energy
cycle. When administered orally to rabbits, ATP increased blood flow, reduced
vascular resistance, and increased arterial oxygen pressure. In baboons, ATP
infusions increased cerebral blood flow by nearly 50 percent and boosted oxygen
consumption in the brain.
Peak ATP™ is a patented brand of ATP that has been tested in human and animal
studies. Peak ATP™ is readily absorbed and boosts circulating ATP levels. Red
blood cells release ATP to produce endothelial vasodilation, or widening of the
arteries. Ensuring adequate red blood cell pools of ATP to help regulate
vascular tone is critical to maintaining circulatory health.
For the first time, Americans have access to proprionyl-L-carnitine and Peak
ATP™, two nutrients that are critical for optimal endothelial function and
structural integrity. |
















